
For years, leaders of the University of Colorado Internal Medicine Residency Program in the Department of Medicine have been brainstorming ways to improve how they train the next generation of doctors.
It was this quest that led to a big change in 2019. The program switched to a new training schedule, called the “4+4 block schedule,” to create more balance in residents’ work hours and opportunities for early, sustained, and personalized career development.
CU faculty conducted research to determine if the new 4+4 block schedule, compared to the previous training schedule as well as national benchmark data, helped improve resident wellness and engagement. Their findings — which were recently published in the Journal of the American Medical Association Network Open — suggest this new model may be associated with substantial improvement in resident burnout and several other positive features.
“The research itself hopefully adds credence to what we’ve done here,” says Daniel Heppe, MD, the first author on the paper and an associate program director in the Internal Medicine Residency Training Program. “I hope that more programs around the country adopt a similar approach so that the improvements we have seen can be more widespread and, ideally, replicated.”
Addressing burnout — a systemic issue
Heppe and his fellow authors define burnout as a work-related syndrome of depersonalization, emotional exhaustion, and low personal achievement, based on the Maslach Burnout Inventory.
Given the long work hours and high-stress scenarios physicians face, burnout can be common. The postgraduate training period is a particularly stressful time for physicians.
“One of the most direct and consistent relationships in this field is between burnout and the number of hours worked,” says Geoffrey Connors, MD, the senior author on the paper and the director of the Internal Medicine Residency Program at the time of the study. “Anywhere one trains, residency will always be the highest sustained period of hours worked that a doctor will experience across their entire career. Given that fact, without intervention, depersonalization, low morale, and all the associated downstream effects are practically to be expected.”
Prior to the COVID-19 pandemic, up to 75% of internal medicine residents at CU showed some symptoms of burnout, according to the research article. One study found 81% of internal medicine residents felt that the pandemic increased their level of burnout.
“Every year, we take 50 incredibly smart, very motivated doctors into our program,” says Connors, who is the future associate dean for Graduate Medical Education and an associate professor in the Division of Pulmonary Sciences and Critical Medicine. “Between medical school and the end of residency, the national pattern is to burn a lot of this high-achieving group out. This means they’re more tired than they were, and they don’t have the same empathy for their patients. It means less healthy doctors and, in turn, doctors who are less likely to have sustained, happy, and productive careers.”
Heppe said mitigating burnout among resident physicians is important because if a resident experiences significant burnout during this time period, it can persist with them for a good portion of their career.
“We are actively interested in making trainees’ experience better, reducing some of these things that are harmful, and producing better physicians to take care of the community at large,” says Heppe, an associate professor in the Division of Hospital Medicine.
One mechanism to address resident burnout is creating a training schedule that allows residents to have more balance between their training rotations, offering them earlier professional development opportunities and more personal time.
“We know that burnout is a systemic problem. It’s not an individual problem,” Connors says. “And so, our thought, at the heart of this, is that a systemic problem requires a systemic solution.”
Changing the schedule
Block scheduling is a method of structuring resident training that is rising in popularity, Connors says.
“The core tenets are that people should have a separation between their inpatient and outpatient responsibilities, so that they can both clinically and educationally focus on one activity at a time,” he says.
For residents, there is a big difference between inpatient and outpatient training in terms of workload. Inpatient training blocks are typically 70-80 hours a week, whereas outpatient and elective training blocks are 40-50 hours a week, Connors says.
Prior to July 2019, the Internal Medicine Residency Program had a 4+1 block schedule, meaning the residents alternated between four weeks of call-heavy, inpatient training rotations and one week of outpatient, ambulatory non-call-focused training rotations.
“I always felt like we could do this better,” Connors says.
The Internal Medicine Residency Program is a three-year program. The first year of residency is referred to as an “intern year.” Historically, interns worked long hours for most of the year because there was an expectation that they had to be mostly independent by the end of the year.
However, that expectation has since changed, which opened the door for the program leaders to re-evaluate the training model.
“To make a great doctor does not mean you have to make a tired doctor. It’s simply not true,” Connors says. “Being well and being well-trained are not mutually exclusive.”
The leaders ultimately decided to implement a 4+4 block schedule, a relatively newer version of block scheduling, Connors says.
Under this model, for all three years, residents do four weeks of inpatient-based training, such as doing rotations in the ICU or hospital wards, which may amount to 80 hours of work per week. These busy four-week blocks are then always followed by four weeks working in a clinic or doing an elective experience. Both of these are just as intellectually rigorous as any inpatient block, but the hours are much better, he says.
“We didn't change the amount of ICU time that our residents do. We didn't change the amount of time they’re on inpatient wards. None of those things went down,” Connors says. “All we did was take this really compressed intern year — that was just busy experience after busy experience — and then we looked at our third year — which was usually two or three busy experiences coupled with people looking for jobs and counterintuitively doing elective career exploration after they had all but chosen a career — and we said, ‘What if we spread both the busyness and the career exploration out over time?’
“Now, each of the years has an equal measure of the really busy inpatient experiences, and the outpatient and elective experiences,” he says. “The best programs see the value in making time for residents to become great bedside doctors while also thoughtfully training them to become medical educators, globalists, researchers, innovators, advocates, and policymakers. That’s not something that you should get lucky to fall into after residency. It should be an intentional part of the training process.”
The hope was that this new training schedule would create more balance for young doctors so they could feel energized as they advance in their careers, while still upholding exceptional training standards.
“Our residents train just as hard as they used to,” Connors says. “But in between those very busy experiences, we are giving time and space for people to do the things that matter to them, which we think is going to improve patient wellness in the future. Great doctors, in our imagining, are well-rounded doctors.”
Research shows value of new schedule
After deciding to switch to the 4+4 block schedule, Heppe and his co-authors conducted research that looked at the association of a 4+4 block schedule — compared to a 4+1 block schedule — with resident wellness, burnout, and self-reported professional engagement and clinical preparedness.
Residents anonymously filled out a survey prior to the block schedule change, assessing burnout, educational outcomes, and quality of life. After the new block schedule was implemented, a second survey was conducted a year later, and a third survey conducted two years later.
The results of the study suggested that the transition to a 4+4 schedule was associated with markedly improved emotional exhaustion and depersonalization domains of burnout.
Residents also reported a positive impact on perceived aspects of professional development, such as job satisfaction and the ability to participate in scholarly activities. Some also noted improved perceived wellness, such as time for friends and family.
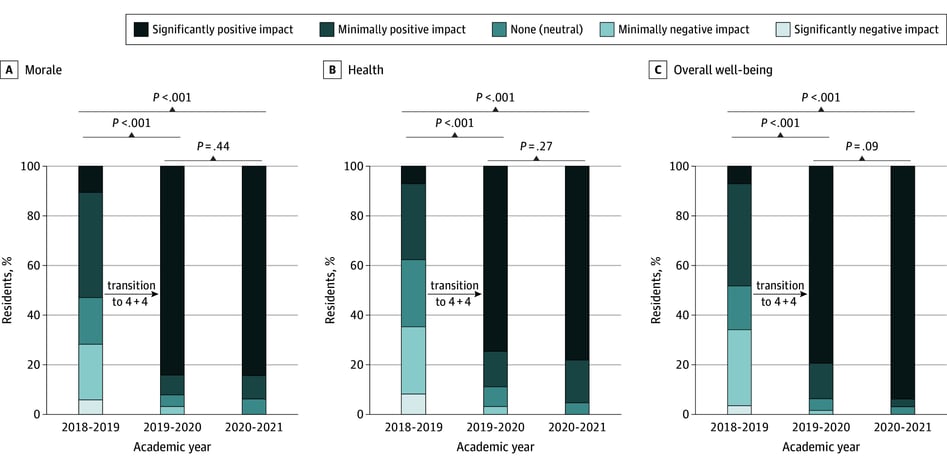 The image above is a figure from the research article. It shows the pre-intervention and post-intervention survey responses from residents regarding perceived impact of the 4+4 block schedule on morale, health, and well-being.
The image above is a figure from the research article. It shows the pre-intervention and post-intervention survey responses from residents regarding perceived impact of the 4+4 block schedule on morale, health, and well-being.
Across multiple years, in-training examination scores showed there was no change in medical knowledge, meaning the residents were still getting the training they needed under this new schedule.
“It shows, on a larger scale, that giving back some amount of agency and time — and spacing out those intense sessions — is good for mental health,” Heppe says.
Connors says he was incredibly pleased to see the results.
“I was most impressed with how quickly a change like this could work,” Connors says. “It was literally one year to the next. The planning was long and hard, but the effect was immediate. This was not something that had to build up. It didn't require momentum. Just giving people that time, in real-time, made a difference in their lives.”
A potential model for others
To the authors’ knowledge, this study is the first to suggest a positive association between the 4+4 block training schedule and internal medicine resident burnout scores.
Given the findings, Heppe and Connors hope the research shows other institutions and programs the potential this 4+4 block schedule model has. Connors says he wants to share this research with other institutions.
“This really could change the national conversation around how we train doctors. I think it is both going to be better for the doctors but also, hopefully, better for the patients,” Connors says. “They’re engaging with doctors who are more thoughtful, less burned out, and more empathic than they might have been otherwise.”
SPECIAL NOTE: We would like to recognize all the authors who contributed to the research paper: Daniel Heppe, MD; Amiran Baduashvili, MD; Julia E. Limes, MD; Katie Suddarth, MD; Adrienne Mann, MD; Emily Gottenborg, MD; Yasmin Sacro, MD; Lisa Davis, MD, MSCS; Karen Chacko, MD; and Geoffrey Connors, MD. The authors would also like to thank the residents who participated in the research and adapted to the block scheduling change.




