When researchers from the University of Colorado Anschutz Medical Campus, Aurora, used a combination of two specific blood-clotting tests, they found critically ill patients infected with Coronavirus Disease 2019 (COVID-19) who were at high risk for developing renal failure, venous blood clots, and other complications associated with blood clots, such as stroke. Their study, which was one of the first to build on growing evidence that COVID-19-infected patients are highly predisposed to developing blood clots, linked blood clotting measurements with actual patient outcomes. The research team is now participating in a randomized clinical trial of a drug that breaks down blood clots in COVID-19-infected patients. “This is an early step on the road to discovering treatments to prevent some of the complications that come with this disease,” said Franklin Wright, MD, FACS, lead author of the research article and an assistant professor of surgery at the University of Colorado School of Medicine. Their research is published as an “article in press” on the Journal of the American College of Surgeons website ahead of print.
Patients who are critically ill regardless of cause can develop a condition known as disseminated intravascular coagulation (DIC). The blood of these patients initially forms many clots in small blood vessels. The body’s natural clotting factors can form too much clot or eventually not be able to effectively form any clot leading to issues of both excessive clotting and excessive bleeding. However, in patients with COVID-19 the clotting appears to be particularly severe and—as evidenced by case studies in China and elsewhere*—clots in COVID-19 patients do not appear to dissipate, explained Dr. Wright.
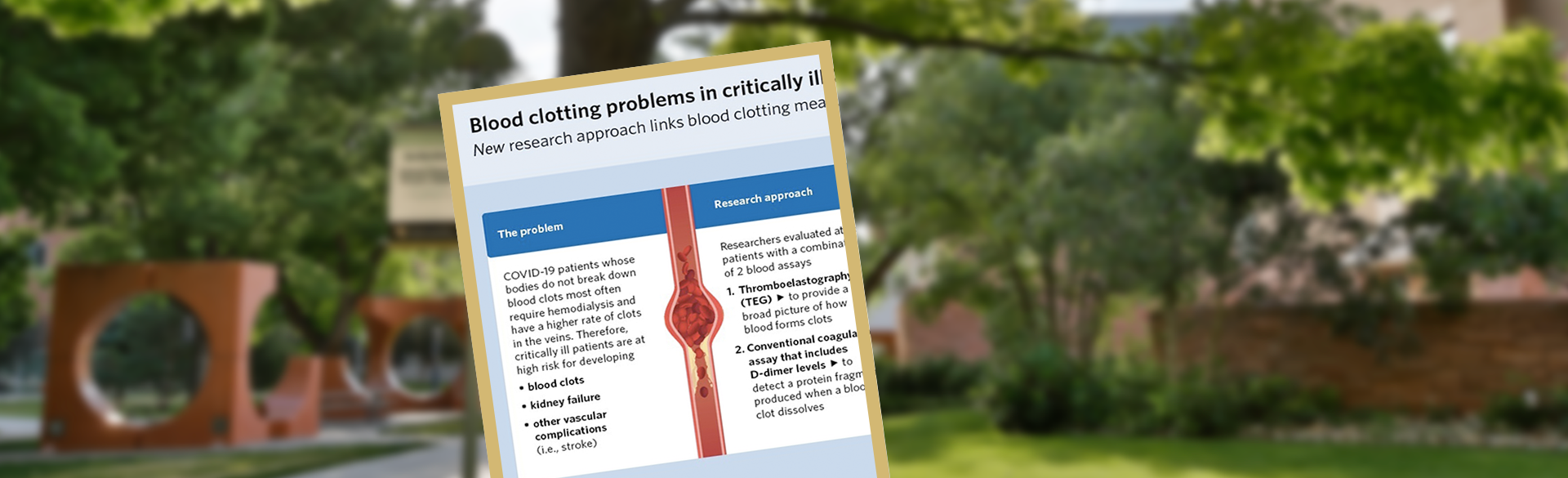
Trauma acute care surgeons and intensive care physicians who treat trauma, transplant, and cardiothoracic surgery patients at UCHealth University of Colorado Hospital saw the potential of using a specialized coagulation test to examine clotting issues in COVID-19 patients. Thromboelastography (TEG) is a whole blood assay that provides a broad picture of how an individual patient’s blood forms clots, including how long clotting takes, how strong clots are, and how soon clots break down. TEG is highly specialized and used primarily by surgeons and anesthesiologists to evaluate the efficiency of blood clotting; it is not widely used in other clinical settings. “The COVID pandemic is opening doors for multidisciplinary collaboration so trauma acute care surgeons and intensivists can bring the tools they use in their day-to-day lives and apply them in the critical care setting to new problems,” Dr. Wright said.
The researchers evaluated outcomes for all patients who had a TEG assay as part of their treatment for COVID-19 infection as well as other conventional coagulation assays, including ones that measure D-dimer levels. D-dimer is a protein fragment that is produced when a blood clot dissolves. D-dimer levels are elevated when large numbers of clots are breaking down.
“These study results suggest there may be a benefit to early TEG testing in institutions that have the technology to identify COVID-19 patients who may need more aggressive anticoagulation therapy to prevent complications from clot formation,” Dr. Wright said.
A total of 44 patients treated for COVID-19 infection between March 22 and April 20 were included in the analysis. Those whose bodies were not breaking down clots most often required hemodialysis and had a higher rate of clots in the veins. These patients were identified by TEG assays showing no clot breakdown after 30 minutes and a D-dimer level greater than 2600 ng/mL. Eighty percent of patients with both affirmative test findings were placed on dialysis compared with 14 percent who tested for neither finding. Patients with affirmative test findings also had a 50 percent rate of venous blood clots compared with 0 percent for those patients with neither finding.
“These study results suggest there may be a benefit to early TEG testing in institutions that have the technology to identify COVID-19 patients who may need more aggressive anticoagulation therapy to prevent complications from clot formation,” Dr. Wright said.
A clinical trial of one form of treatment is already underway. The Denver Health and Hospital Authority is leading a multi-center study that includes UCHealth University of Colorado Hospital, National Jewish Health-St Joseph Hospital, Beth Israel Deaconess Medical Center, and Long Island Jewish Hospital in conjunction with Genentech, Inc., enrolling patients with COVID-19 infection in a randomized clinical trial of tissue plasminogen activator (tPA). This drug is a clot-busting, thrombolytic medicine that was first approved by the U.S. Food and Drug Administration in 1987 for the treatment of heart attack and later approved for acute massive pulmonary embolism and acute ischemic stroke. The trial will assess the efficacy and safety of intravenous tPA in improving respiratory function and management of patients with aggressive blood clotting.
“This study suggests that testing whole blood clotting measurements may allow physicians to identify and treat patients with COVID-19 more effectively to prevent complications and encourage further research into therapies to prevent blood clots in these patients,” Dr. Wright said.
Dr. Wright’s associates in this study include: Thomas O. Vogler, PhD; Ernest E. Moore, MD, FACS; Hunter B. Moore, MD, PhD; Max V. Wohlauer, MD; Shane Urban, BSN, RN; Trevor L. Nydam, MD, FACS; Peter K. Moore, MD; and Robert C. McIntyre Jr., MD, FACS.
YouTube links:
- https://www.youtube.com/watch?v=KMduQQMTv_s&feature=youtu.be
- https://www.youtube.com/watch?v=6OtSCR6rFwE&feature=youtu.be
Guest Contributor: Journal of the American College of Surgeons


