Immunotherapies have revolutionized the care of many cancers, teaching the body’s own immune cells to recognize and attack tumor cells. Leading the way are drugs known as checkpoint inhibitors, which block a kind of “white flag” that tumors wave as a peace signal to T cells that would very much like to kill them. Really, this white flag is a protein called PD-L1 – many tumors coat themselves in it. When PD-L1 on the surface of a cancer cell sees its partner, PD1, on T cells, these T cells are tricked into letting the cancer cell live. To counteract this dirty trick, checkpoint inhibitor drugs block the functions of PD-L1 on tumor cells (e.g. atezolizumab) or PD1 on T cells (e.g. pembrolizumab), allowing T cells to go about their cancer-killing business.
Unfortunately, checkpoint inhibitors don’t work all the time. For reasons that have been largely unknown, some patients respond to checkpoint inhibitor therapies, while others do not. A University of Colorado Cancer Center study published in the journal Cancer Immunology Research offers insight and possibly an inroad into this problem: In mouse models of B-cell lymphoma, adding another drug, called a histone deacetylase (HDAC) inhibitor, sensitized cancers to anti-PD1 therapy.
“I think this combination is definitely worth trying,” says Jing Wang, MD, PhD, investigator at CU Cancer Center and associate professor in the CU School of Medicine Department of Immunology and Microbiology.
The reason this combination works is a bit complex. However, it may help to explain not only why some patients fail to respond to anti-PD1 immunotherapy, but also why HDAC inhibitors, which have seemed so promising in the lab, have been largely unsuccessful with patients.
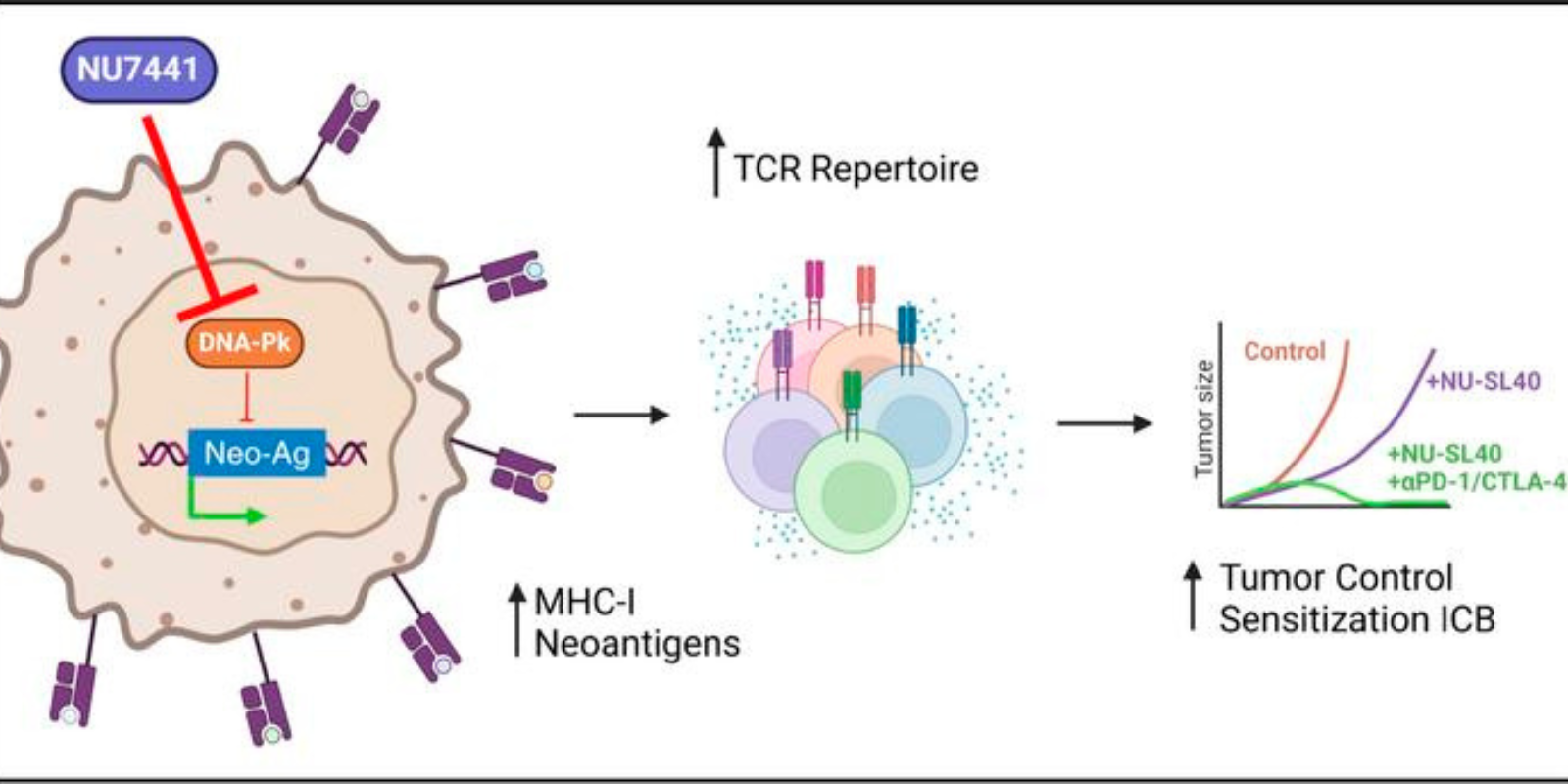
The reason has to do with another set of proteins, called major histocompatibility complex (MHC). In fact, MHC describes a few classes of proteins – think of them like silver platters, only in this case, instead of serving food, MHC proteins serve antigens. Basically, MHC proteins grab and little bits of proteins from inside a cell and present them on the cell surface for inspection by our T cells. And when our T cells recognize a dangerous antigen sitting on an MHC platter, they attack that cell (you know, unless the T cell is deactivated by the PD1/PD-L1 interaction).
If a cancer cell has no MHC proteins, it doesn’t matter if immunotherapy blocks the PD1/PD-L1 interaction – without MHC, the cancer cell presents no antigens and so the immune system sees no danger.
“T cells recognize antigens in the context of MHC. Without MHC, you can’t present an antigen. And about 60 percent of diffuse large B cell lymphomas downregulate MHC,” Wang says.
This is one side of the story: Anti-PD1 immunotherapies may not work in cancers that downregulate MHC. Here is the other side: It appears that the class of drugs known as HDAC inhibitors upregulate MHC. Specifically, the study showed that the experimental HDAC inhibitor OKI-179 (provided by OnKure Therapeutics, Inc. and currently in a phase 1 clinical trial at CU Cancer Center) was like a switch: Without OKI-179, the group’s models of B-cell lymphoma resisted anti-PD1 therapy; with OKI-179 added to anti-PD1 therapy, cancer cells were killed.
“We treated our mouse model of B-cell lymphoma with this HDAC inhibitor. The inhibitor alone had some effect, but when we combined it with anti-PD1 it worked a lot better. Dual inhibition – both HDAC and PD1 – achieved a better effect,” Wang says.
Finally, the study may help to explain why previous HDAC inhibitors have struggled. Remember, there are two systems at work – the PD1/PD-L1 interaction (which is bad) and also MHC proteins that present antigens (which is good). HDAC inhibitors may upregulate MHC proteins (again, this is good), but the current study shows that HDAC inhibitors may also upregulate PD-L1, helping cancer cells to pepper themselves with these white flags that deactivate the immune system (which is bad).
Now imagine this solution: An HDAC inhibitor upregulates MHC and as an unfortunate byproduct upregulates PD-L1… but an anti-PD1 checkpoint inhibitor nixes the immune system’s ability to recognize all this extra PD-L1. The HDAC inhibitor restores MHC, serving more antigens to T cells, making the anti-PD1 therapy work better; and the anti-PD1 therapy keeps our T cells from recognizing any extra PD-L1 on cancer cells, making the HDAC inhibitor work better. In this scenario, the combination of HDAC inhibitor with anti-PD1 is greater than the sum of each drug used alone.
“We think this immunologic effect is very important. This paper emphasizes the immunologic action of HDAC. If your HDAC inhibitor is upregulating PD-L1, you’re not going to make it work alone. But if you also block PD1, HDAC inhibition looks much more successful,” Wang says.
At least that’s the theory. Ongoing work continues to explore the promise of this combination in systems closer to human cancer.