Search for:
Submit
Submit
Webmail
UCD Access
Canvas
Quick Links
Tools & Resources
Events Calendar
Newsroom
Strauss Health Sciences Library
Department A-Z Directory
Campus Directory
Leadership
Faculty & Staff Resources
Supporter & Alumni Resources
Student Resources
Mental Health Resources
Campus Map
University Policies
Give Now
CU Campuses
CU Anschutz
CU Boulder
CU Colorado Springs
CU Denver
CU System
CU Online
CU Anschutz
School of Dental Medicine
Graduate School
School of Medicine
College of Nursing
Skaggs School of Pharmacy and Pharmaceutical Sciences
Colorado School of Public Health
Cancer Center
Home
About Us
Director's Message
Cancer Center Leadership
Cancer Center Staff
National Cancer Institute-Designated Comprehensive Cancer Center
National Comprehensive Cancer Network
Partnerships
Staff and Member Resources
Contact Us
Make a Gift
Patients & Families
Cancers We Treat
Cancer Screening
Multidisciplinary Clinics
Second Opinions
Supportive Care
Survivorship
Genetic Counseling
Clinical Trials
Clinical Research
Investigator-Initiated Trials
Research
Funding Opportunities
Members
Research Partners
Research Programs
Scientific Focus Groups
Shared Resources
Education
K-12 Training & Education Opportunities
Undergraduate & Post-Baccalaureate Training & Education Opportunities
Graduate, Post-Doctoral, & Medical Student Training & Education Opportunities
Junior Faculty Professionals
Training Grants
Community
Office of Community Outreach and Engagement
News
Events
Cancer
Cancer
Celebrating Strength and Hope: A National Cancer Survivor’s Day 2026 Reflection
by Megan Palffy
| June 05, 2026
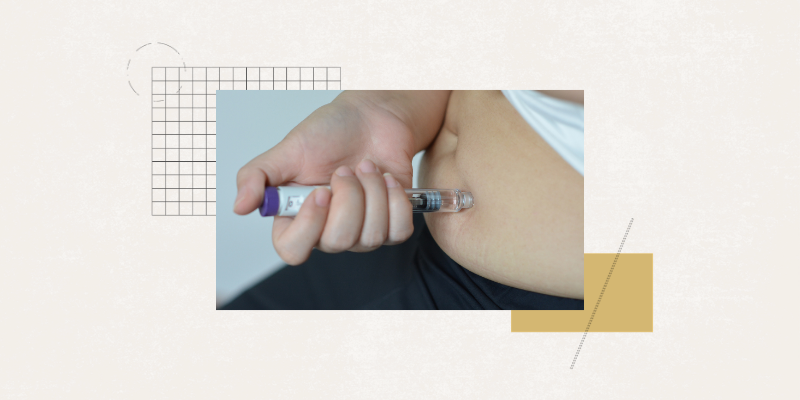
Cancer
Can GLP-1 Drugs Boost Immunity?
by Greg Glasgow
| May 26, 2026
Cancer
Meeting the Special Needs of Adult Survivors of Childhood Cancer
by Mark Harden
| April 13, 2026
Cancer
What Are Targeted Cancer Therapies?
by Mark Harden
| March 17, 2026
Cancer
A Guide to Imaging Technologies that Revolutionized How Cancer is Diagnosed and Treated
by Mark Harden
| March 04, 2026
Cancer
What Genetic Testing Can Reveal about Hereditary Cancer Conditions
by Mark Harden
| February 28, 2026
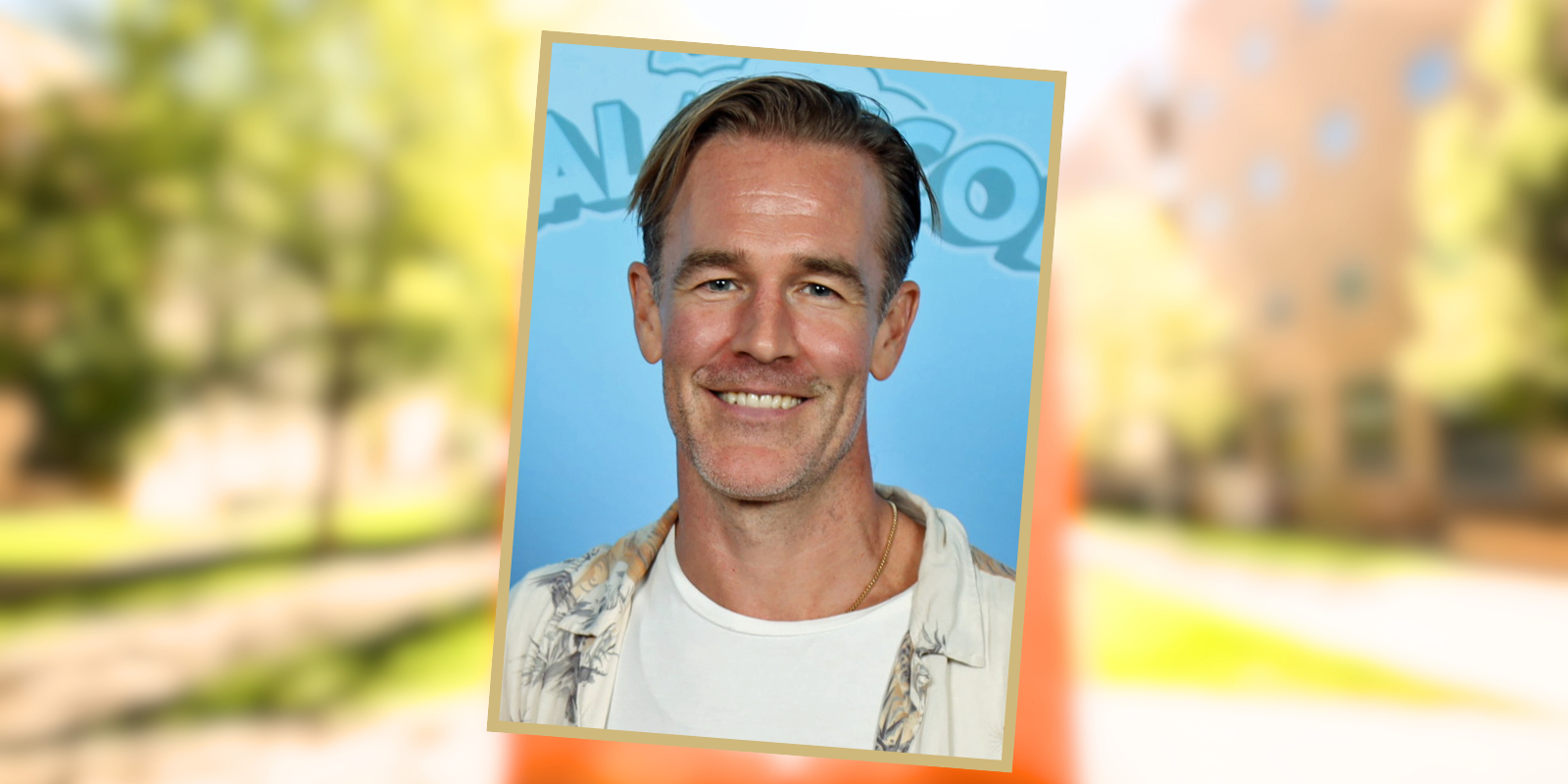
Cancer
'You're Never Too Young': CU Anschutz Cancer Center Expert on James Van Der Beek’s Colorectal Cancer
by Mark Harden
| February 11, 2026
Cancer
CU Cancer Center Top Stories of 2025
by Cancer Center
| December 15, 2025
Cancer
What to Know About ‘Full House’ Actor Dave Coulier’s Oropharyngeal Cancer
by Mark Harden
| December 04, 2025
Cancer
In a Holiday Conversation About Cancer, What You Don’t Say Matters
by Mark Harden
| November 25, 2025
Cancer
What Are the Big Unanswered Questions About Cancer? We Asked the Experts.
by Mark Harden
| November 13, 2025
Cancer
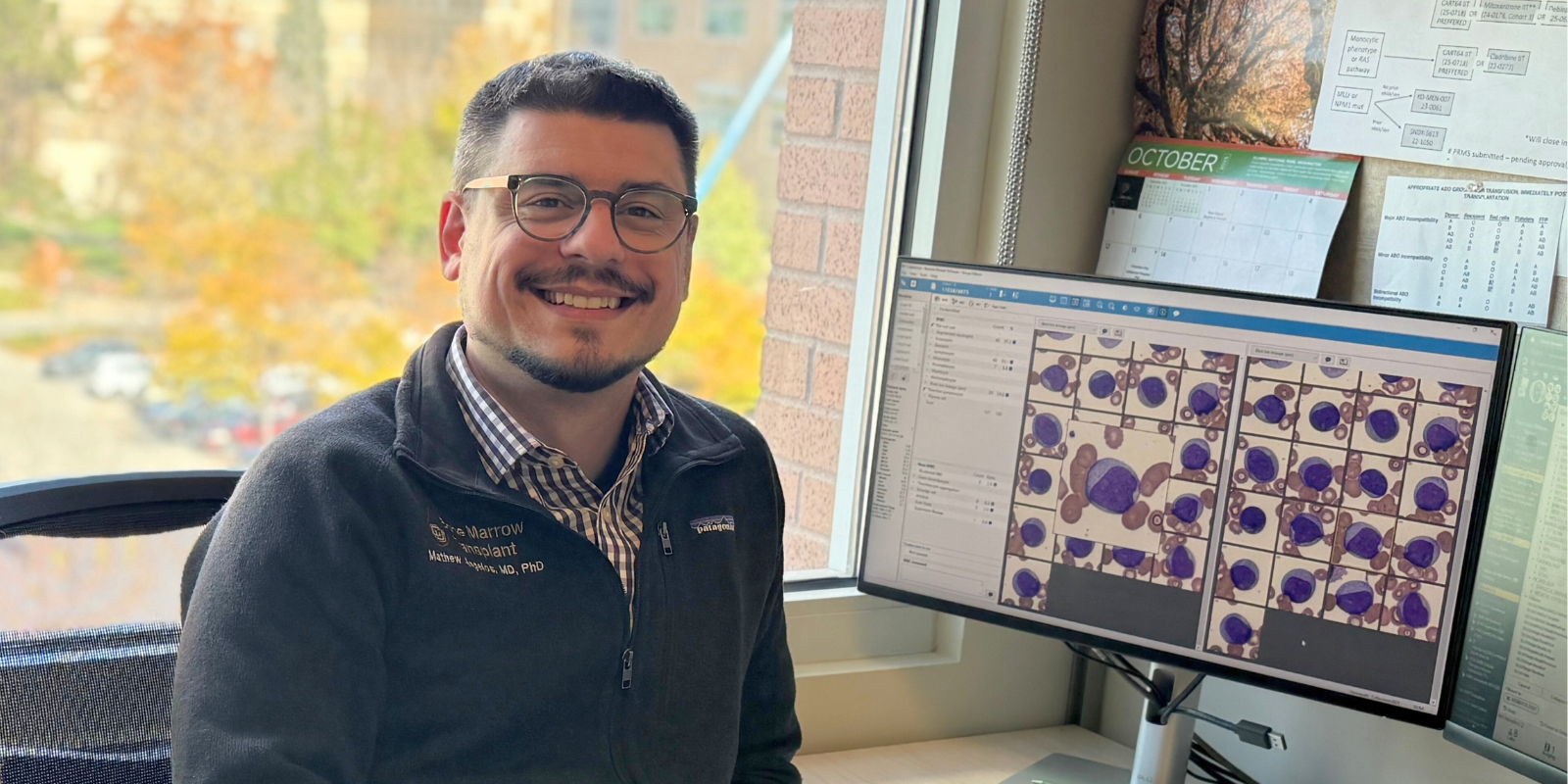
A New Arrival at CU Cancer Center Tests a Homegrown Treatment for Aggressive Leukemia
by Mark Harden
| November 12, 2025
Cancer
Why Palliative Care Goes Hand in Hand with Treatment for People with Cancer
by Mark Harden
| November 10, 2025
Cancer
A New Playbook for Assessing Older Patients With Cancer in Places Where Resources are Scarce
by Mark Harden
| October 23, 2025
Cancer
Eyes Widen for Uveal Melanoma Treatment: Sapna Patel’s Groundbreaking Findings at ESMO 2025
by Megan Palffy
| October 21, 2025
Cancer
Debunking 8 Myths About Cancer Clinical Trials
by Mark Harden
| October 06, 2025
Cancer
Exploring How Cancer-Fighting Cells Get Reprogrammed to Help Cancer Grow
by Mark Harden
| August 19, 2025
Cancer
Why Should You Consider a Cancer Clinical Trial? Here Are Answers from a CU Cancer Center Leader.
by Mark Harden
| July 03, 2025
Cancer
A Research Roadshow Brings the CU Cancer Center to a Cancer-Challenged Community
by Mark Harden
| June 19, 2025
Cancer
40 Years of Preventing and Conquering Cancer
by Mark Harden
| June 05, 2025
Cancer
‘Building Bridges’: The CU Cancer Center Names Four Program Liaisons
by Mark Harden
| May 20, 2025
Cancer
‘We’re Your Family’: New Clinic Helps Diagnose Patients with Suspected Cancer
by Mark Harden
| May 08, 2025
Cancer
More Cancer Patients Learn About Clinical Trials Through a CU Cancer Center Project
by Mark Harden
| May 07, 2025
Cancer
Telehealth Program Targets Severe Sleeplessness Among Colorado Cancer Patients
by Mark Harden
| April 03, 2025
Cancer
New CAR-T Cell Therapy Shows Promise for Hard-to-Treat Cancers
by Laura Kelley
| March 10, 2025
Cancer
CU Cancer Center Leaders Applaud Denver’s Ban on Flavored Tobacco Sales
by Mark Harden
| February 10, 2025
Cancer
A CU Cancer Center Member’s Visit to a Colorado Industrial City Inspires Research into Heavy Metals’ Impact
by Mark Harden
| January 29, 2025
Cancer
Alcohol is a Leading Cause of Cancer, But Will the Public Heed a New Warning?
by Mark Harden
| January 08, 2025
Cancer
Oncology Hospitalists Deliver Better Care to Cancer Patients in the Hospital
by Mark Harden
| December 16, 2024
Cancer
‘The Opportunities Are Endless’: CU Cancer Center Leader Signs Key International Agreement
by Mark Harden
| December 10, 2024
Cancer
Part of the Solution: Grateful Blood Cancer Patient Supports CU Cancer Center Research
by Mark Harden
| November 22, 2024
Cancer
A Global Perspective on Indigenous Peoples and Cancer
by Mark Harden
| November 15, 2024
Cancer
News to Use: What to Know About Breast Cancer
by Mark Harden
| November 11, 2024
Cancer
Renowned CSU Research Center Fights Cancer in Both Pets and People
by Mark Harden
| November 04, 2024
Cancer
‘These Are Things You’ve Got to Talk About’: How Cancer Impacts Hispanic Coloradans
by Mark Harden
| October 02, 2024
Cancer
CU Cancer Center Scientific Retreat Spotlights Successes, Challenges
by Mark Harden
| September 30, 2024
Cancer
Despite Advances, Breast Cancer Remains the Number 1 Cancer Among Women
by Mark Harden
| August 19, 2024
Cancer
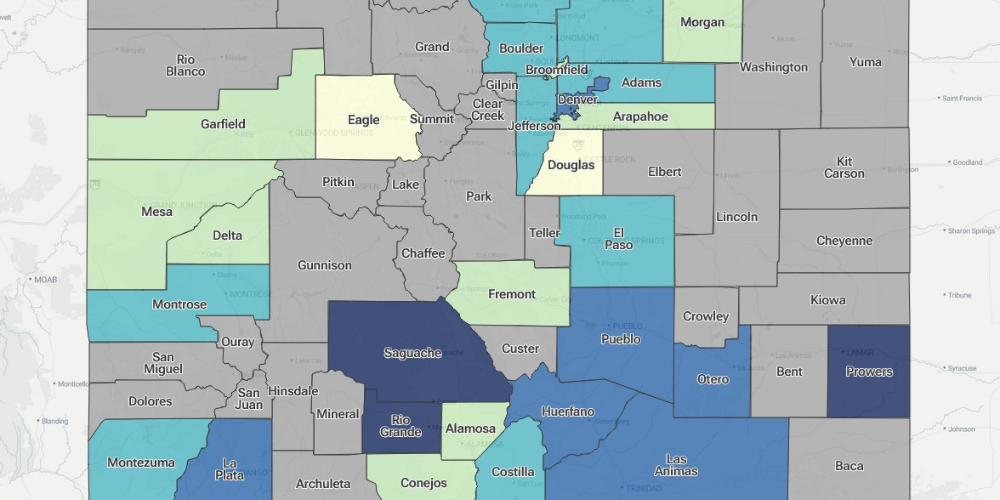
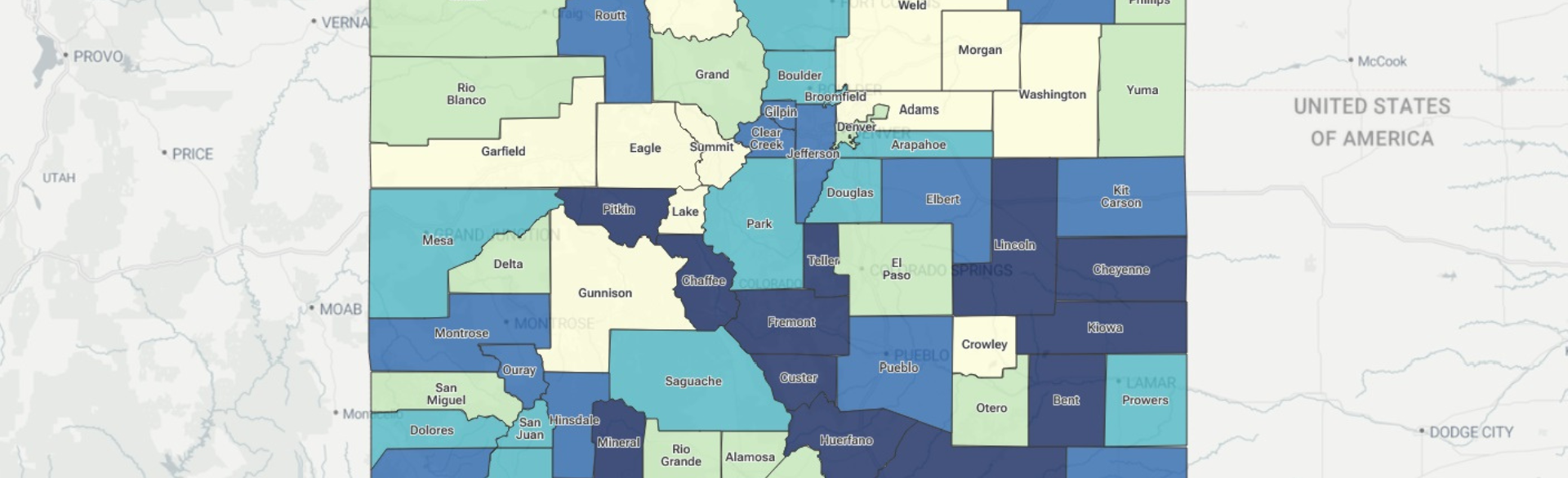
Introducing an Interactive Mapping Tool to Display Colorado Cancer Data
by Mark Harden
| August 12, 2024
Cancer
Helping Patient Navigation Programs Become Sustainable
by Greg Glasgow
| July 01, 2024
Cancer
‘An Obligation to Make Things Better’: Coping With Cancer Disparities Among LGBTQ+ Communities
by Mark Harden
| June 26, 2024
Cancer
Addressing Cancer Disparities Among Minorities is a Mission for the CU Cancer Center
by Mark Harden
| April 01, 2024
Cancer
‘We’re All In This Together’: CU Cancer Center Leaders Share Insights With Colorado Legislators
by Mark Harden
| February 07, 2024
Cancer
Toby Keith’s Death Following Stomach Cancer Fight Brings Attention to a Less Common Cancer
by Rachel Sauer
| February 06, 2024
Cancer
You Just Got a Cancer Diagnosis. Should You Get a Second Opinion?
by Mark Harden
| February 01, 2024
Cancer
U.S. Expected to Break Annual Record for New Cancer Cases; Colorectal Cancer Risk Looms for Under-50 Americans
by Mark Harden
| January 17, 2024
Cancer
What to Know About Supportive Care Trials
by Mark Harden
| December 12, 2023
Cancer
CU Cancer Center Was the Right Destination for a Lifelong Outdoorsman with Pancreatic Cysts
by Mark Harden
| November 22, 2023
Cancer
Research Offers Insight into Improving Efficacy of PD-L1 Immunotherapy for Cancer Patients
by Julia Milzer
| July 06, 2023
Cancer
Understanding Cancer in the Mind and the Heart
by Rachel Sauer
| June 05, 2023
Cancer
Where Advanced Cancer Patients Are Discharged After Hospitalization Affects Outcomes
by Rachel Sauer
| April 12, 2023
Cancer
Growing Health and Wellness in the Community Garden
by Rachel Sauer
| March 28, 2023
Cancer
Most People Diagnosed with Cancer Seek Information Even Before Their Appointments
by Rachel Sauer
| February 13, 2023
Cancer
Research Illuminates a Therapeutic Strategy to Induce Cancer Cell Death
by Rachel Sauer
| February 10, 2023
Cancer
New Drug Combination Might Better Treat Often Fatal Childhood Brain Tumor
by Laura Kelley
| January 19, 2023
Cancer
Study Finds New Feature Indicative of Gastrointestinal Tumor Recurrence
by Kelsea Pieters
| January 09, 2023
Cancer
Using Big Data to Help Understand when a Treatment is Right for Prostate Cancer Patients
by Rachel Sauer
| January 09, 2023
Cancer
CU Cancer Center Top Stories of 2022
by Cancer Center
| December 19, 2022
Cancer
Women Are Gaining Increasing Seats at the Table in Cancer Leadership
by Rachel Sauer
| November 28, 2022
Cancer
CU Anschutz Researchers Find Less Invasive Treatment for Certain Head and Neck Cancers
by Kelsea Pieters
| November 28, 2022
Cancer
Selective Nodal Radiation May Be a More Effective Approach in Cancer Treatment
by Laura Kelley
| November 16, 2022
Cancer
Focusing on Cancer, Work, and Employment
by Rachel Sauer
| November 16, 2022
Cancer
The Message Hasn’t Changed: Get Colorectal Cancer Screening
by Rachel Sauer
| October 13, 2022
Cancer
R01 Grant Supports Deep Dive into Protein Associated with Cachexia in Late-Stage Colorectal Cancer
by Rachel Sauer
| September 30, 2022
Cancer
Ongoing Research Studying Effect of High-Dose Testosterone in Treating Prostate Cancer
by Rachel Sauer
| September 28, 2022
Cancer
Cancer Physical Medicine and Rehabilitation an Important Aspect of Patient-Centered Care
by Rachel Sauer
| September 23, 2022
Cancer
Studying Psychedelics to Treat Psychiatric Distress in Late-Stage Cancer
by Rachel Sauer
| August 15, 2022
Cancer
Newly Developed Reference Chart Helps Monitor Cancer-Related Fatigue Improvements Through Exercise Program
by Rachel Sauer
| July 29, 2022
Cancer
American Cancer Society Supports CU Cancer Center Researchers with Almost $2 Million in Grant Funding
by Rachel Sauer
| July 01, 2022
Cancer
CU Cancer Center Researchers Receive AB Nexus Grant Support for Intercampus Collaboration
by Rachel Sauer
| June 24, 2022
Cancer
Four Collaborative Human/Canine Cancer Research Projects Receive Pilot Grant Funding
by Rachel Sauer
| May 26, 2022
Cancer
Early Days of COVID-19 Pandemic Brought Increased Anxiety for Some Cancer Survivors
by Rachel Sauer
| May 16, 2022
Cancer
Understanding Metastasized Cancer
by Rachel Sauer
| May 04, 2022
Cancer
Drug Developed in CU Lab Shows Promise Against a Novel Oncogene that Supports Cancer Progression
by Rachel Sauer
| April 04, 2022
Cancer
6 Years After Bile Duct Cancer Diagnosis, Focus Shifts to Not Wasting Time
by Rachel Sauer
| February 22, 2022
Cancer
Cancer Clinical Trials Office Welcomes New Medical Director
by Rachel Sauer
| February 11, 2022
Cancer
Molecular and Cellular Oncology Program Co-Leaders Focus on Growing Diversity, Equity, and Inclusion in Research
by Rachel Sauer
| December 22, 2021
Cancer
New Program Leadership at the CU Cancer Center
by Rachel Sauer
| December 10, 2021
Cancer
Research Demonstrates that Cells with Cancer-Associated Mutations Overtake Human Tissue with Age
by Rachel Sauer
| December 03, 2021
Cancer
Association of Community Cancer Centers Names Innovator Award Recipients
by Healio
| November 06, 2021
Cancer
‘Coming Out’ to Cancer: LGBTQIA+ Discrimination in the Health Care System
by Cure Today
| November 05, 2021
Cancer
Innovative Ovarian Cancer Research Newly Supported by R37 MERIT Award
by Rachel Sauer
| September 13, 2021
Cancer
CU Cancer Center Celebrates National Cancer Survivors Day
by Cancer Center
| June 01, 2021
Cancer
May Is National Cancer Research Month
by Cancer Center
| May 06, 2021
Cancer
Start the Conversation About Fertility Preservation Before Beginning Cancer Treatment
by Jessica Cordova
| August 10, 2020
Cancer
Multi-organizational study aims to improve outcomes of minority children with brain and central nervous system tumors
by Cancer Center
| August 04, 2020
Cancer
Cancer Doesn't Stop for a Pandemic
by Cancer Center
| July 17, 2020
Cancer
Reversing a Miracle
by Cancer Center
| July 16, 2020
Cancer
To Live: Artist Shelley Kerr’s Sculptures Explore the Battle, Journey and Gratitude of Five Years With Stage IV Cancer
by Cancer Center
| July 16, 2020
Cancer
Building Towards Early Detection of Ovarian Cancer
by Cancer Center
| July 16, 2020
Cancer
What is Sarcoma?
by Cancer Center
| July 01, 2020
Cancer
CU Cancer Center Study Aims to Increase Access to Head and Neck Cancer Clinical Trials in Hispanic Population
by Cancer Center
| June 29, 2020
Cancer
CU Cancer Center study tackles racial and socioeconomic disparities in patients with lung cancer
by Cancer Center
| June 24, 2020
Cancer
CU Cancer Center Researcher Named Pew-Stewart Scholar Aims to Improve Early Cancer Detection
by Cancer Center
| June 15, 2020
Cancer
Chad Rusthoven, MD, awarded Coltman Fellowship to support small-cell lung cancer research
by Cancer Center
| June 08, 2020
Cancer
Cord blood as source for stem cell transplant may outperform accepted “gold standard” of matched sibling donors
by Cancer Center
| June 08, 2020
Cancer
National Cancer Survivors Awareness Day 2020
by Cancer Center
| June 07, 2020
Cancer
FIRE-SCLC analysis: Largest ever study of first-line radiosurgery for brain metastases from small cell lung cancer
by Cancer Center
| June 04, 2020
Cancer
Oncology nurse turned cancer survivor is dedicated to improving the quality of care for patients
by Cancer Center
| June 01, 2020
Cancer
Colorado tool, My-DST, may pick best multiple myeloma treatment
by Cancer Center
| May 28, 2020
Cancer
Do chemicals in sunscreen cause cancer?
by Cancer Center
| May 28, 2020
Cancer
D. Ross Camidge, MD, PhD: COVID-19 lung cancer treatment diary
by Cancer Center
| May 14, 2020
Cancer
Variation in how side effects are reported leaves first impressions of new anti-cancer drugs open to manipulation
by Cancer Center
| April 28, 2020
Cancer
What Patients Should Know About Anti-Cancer Immunotherapy Side Effects
by Cancer Center
| March 17, 2020
Cancer
Humans of Anschutz: Heather Leach, PhD
by Cancer Center
| March 09, 2020
Cancer
COVID-19 Recommendations for Cancer Patients
by Cancer Center
| March 05, 2020
Cancer
University of Colorado Cancer Center adds years back to bile duct cancer patient’s life
by Cancer Center
| February 27, 2020
Cancer
Community climbing competition raises funds for CU Cancer Center research
by Cancer Center
| February 17, 2020
Cancer
What is Cancer?
by Cancer Center
| February 11, 2020
Cancer
Colorado’s James DeGregori, PhD, to lead new journal ‘Aging and Cancer’
by Cancer Center
| January 30, 2020
Cancer
Study Shows Lactate May Prompt Cancer Formation
by Cancer Center
| January 15, 2020
Cancer
Prevent and Conquer Cancer. Together.
by Cancer Center
| January 09, 2020
Cancer
Plant-derived SVC112 hits cancer stem cells, leaves healthy cells alone
by Cancer Center
| January 08, 2020
Cancer
CU Cancer Center Annual Retreat and Poster Session presents cutting-edge research
by Cancer Center
| November 06, 2019
Cancer
$2M award helps CU startup build new tech to find better cancer drugs
by Cancer Center
| October 30, 2019
Cancer
Rural Colorado missing out on cancer prevention, detection, and care. Now, $4.2M project seeks to change that.
by Cancer Center
| October 10, 2019
Cancer
Jason Quinn, MBA/MHA joins CU Cancer Center as Assistant Director of Operations
by Cancer Center
| October 08, 2019
Cancer
Will you go Over the Edge with James DeGregori, PhD, to help the Cancer League of Colorado?
by Cancer Center
| October 02, 2019
Cancer
American Cancer Society research breakfast highlights Colorado discoveries changing the face of cancer care
by Cancer Center
| October 01, 2019
Cancer
Closing the mental health care gap for cancer patients
by Cancer Center
| September 25, 2019
Cancer
Nobel Laureate, Tom Cech, PhD, suggests new way to target third most common oncogene, TERT
by Cancer Center
| September 10, 2019
Cancer
Cancer League of Colorado Matches Gifts Through Sept 30th
by Cancer Center
| September 05, 2019
Cancer
Evelinn Borrayo, PhD, brings experience, ideas to healing the cancer care divide in Colorado
by Cancer Center
| September 04, 2019
Cancer
New immune system understanding may help doctors target cancer
by Cancer Center
| August 20, 2019
Cancer
$4M grant aims to reduce stress in cancer caregivers
by Cancer Center
| August 19, 2019
Cancer
Biotech fieldtrip helps CU Research Summer Fellowship Program students explore range of career options
by Cancer Center
| August 15, 2019
Cancer
Denver Over the Edge: Rappel a skyscraper to raise money for cancer research!
by Cancer Center
| August 14, 2019
Cancer
$1.6M grant will help CU Cancer Center Summer Research Fellowship Program increase diversity and innovation
by Cancer Center
| August 08, 2019
Cancer
Support Colorado Cancer Research at Race 4 Research!
by Cancer Center
| July 19, 2019
Cancer
National Cancer Institute grant helps speed process of Colorado clinical trials
by Cancer Center
| July 18, 2019
Cancer
Ben Walburn: All the Time in the World
by Cancer Center
| July 02, 2019
Cancer
CU Cancer Center Deputy Director, Cathy J. Bradley, PhD, earns grant to close urban-rural cancer care gap
by Cancer Center
| June 26, 2019
Cancer
How human genetic data could help dogs fight cancer
by Cancer Center
| June 25, 2019
Cancer
God doesn’t play dice. Does cancer?
by Cancer Center
| June 20, 2019
Cancer
Cancer care providers see benefit in medical marijuana, but not comfortable prescribing
by Cancer Center
| May 28, 2019
Cancer
Former and current CU Cancer Center Directors, Bunn and Schulick, describe how research and philanthropy will beat cancer
by Cancer Center
| May 14, 2019
Cancer
The genetic diversity that may explain differences in cancer rates across ethnicities
by Cancer Center
| May 13, 2019
Cancer
Scientists at CU Cancer Center receive awards for childhood cancer research
by Cancer Center
| April 30, 2019
Cancer
CU Cancer Center leaders visit AstraZeneca to discuss speeding drug development efforts
by Cancer Center
| April 18, 2019
Cancer
Three Colorado studies show how tumors hijack the immune system to resist radiation therapy
by Cancer Center
| April 16, 2019
Cancer
Irinotecan breaks cancer cell DNA – AZD0156 keeps the body from repairing it
by Cancer Center
| April 03, 2019
Cancer
AACR: Tobacco use makes precancerous cells that “fertilize” cancer growth
by Cancer Center
| April 01, 2019
Cancer
Adavosertib speeds cancer cells into the wall of mitotic catastrophe
by Cancer Center
| April 01, 2019
Cancer
Colorado drug takes aim at cancer metastasis
by Cancer Center
| April 01, 2019
Cancer
CU Cancer Center program recognized at Colorado Capitol
by Cancer Center
| March 28, 2019
Cancer
Inspiring the Next Cancer Scientists
by Taylor Abarca
| February 27, 2019
Cancer
Young Adult Cancer Survivors Struggle with Debt, Work-Related Impairments
by Garth Sundem
| February 25, 2019
Cancer
The State of Cancer in Colorado
by Garth Sundem
| February 04, 2019
Cancer
“No One Hates Cancer More Than I Do”
by Garth Sundem
| January 03, 2019
Cancer
Karyn Goodman, MD, Named Co-Chair of NCI Gastrointestinal Cancer Steering Committee
by Garth Sundem
| October 15, 2018
Cancer
Cancer Hijacks the Microbiome to Glut Itself on Glucose
by Garth Sundem
| September 28, 2018
Cancer
Innovative Cancer Immunology Researcher Joins CU Cancer Center
by Kelli Jones
| September 04, 2018
Cancer
Richard Schulick Named Director of University of Colorado Cancer Center
by Mark Couch
| June 07, 2018
Cancer
In Breast Surgery, Sometimes Less is More
by Garth Sundem
| December 07, 2017
Cancer
Immunotherapy: A Love Story
by UCHealth
| August 10, 2017
Cancer
Malaria Drug Successfully Treats 26-year-old Brain Cancer Patient
by Garth Sundem
| January 17, 2017
Cancer
New Drug Trial Shows Promise in Fighting Cancer for CO Woman
by 9News
| September 14, 2016
Cancer
Former NCAA Basketball Player Calls CU Cancer Center Home
by Taylor Abarca
| April 12, 2016
Cancer
EBRT with Brachytherapy Offers Modest Survival Benefit in Prostate Cancer
by Garth Sundem
| February 08, 2016
Cancer
Cannabis & Cancer: Cause, Cure, Conundrum
by Garth Sundem
| December 14, 2015
Cancer
Dietary Supplements Shown to Increase Cancer Risk
by Garth Sundem
| April 20, 2015
Cancer
After Great Dane Success, Cancer Doc Eyes Brain Tumors
by Garth Sundem
| June 27, 2013
Load more