How are dentures currently made?
The majority of dentures are still what we call analog dentures which have been used in dentistry for a very long time. They take a significant amount of time to produce and that process involves a lot of labor intensive steps.
Conventional denture fabrication involves multiple steps with several transitions, all of which introduce potential dimensional changes and distortions.
We have to do relining and adjustments to get the right final shape, so it’s easy to see how people can have problems with dentures fitting.
What are traditional denture teeth made of?
The teeth can be made of different materials.
- Acrylic: These are budget options – injection molded and made from a material called polymethylmethacrylate or composite resins similar to what a dentist uses to fill a cavity in a natural tooth. They can wear relatively rapidly, leading to a degradation of fit and not having the right occlusion (contact between teeth), which impacts both speech and chewing.
- Porcelain or other ceramics: These are the more expensive option and they can provide a more natural tooth esthetic than acrylics. They are strong but very brittle – a small drop could chip a tooth that may or may not be repairable. Ceramic is also heavier than acrylic and you feel that weight in your mouth.
Still, either of these treatment options are better for overall health than not restoring the dentition.
What are the different types of dentures?
Partial and complete.
Patients who are edentulous (have lost all natural teeth) need a different restorative solution than patients who have retained some teeth and can be treated using a partial denture, where you fill in only the missing teeth. Typically, there's a clasp that locks onto the remaining teeth.
Complete dentures can be fixed in place or removable. If it's fixed, there are typically four implants locking that denture in place.
Despite all the hurdles, how do current dentures still protect health?
Dentures enhance the quality of life for patients by making it easier to speak and to chew food. Patients without teeth or a denture may be essentially consuming soft foods and that can make eating a balanced diet more difficult and staying healthy challenging.
How much do current dentures cost?
We want the best outcomes for patients and part of that conversation needs to be about affordability.
Denture care requires diagnostic procedures and procedures to restore health to oral tissues before fabricating the dentures. The costs associated with procedures necessary to prepare a patient for dentures along with the processes for fabricating them can vary widely depending upon many circumstances and can be in the thousands of dollar range. That’s why we’re so interested in 3D printing for dentures – the materials can be significantly less expensive and the process is more efficient and more affordable than analog or milled dentures.
What’s the current state of 3D printing in dentistry? What is the difference in how a patient is initially examined?
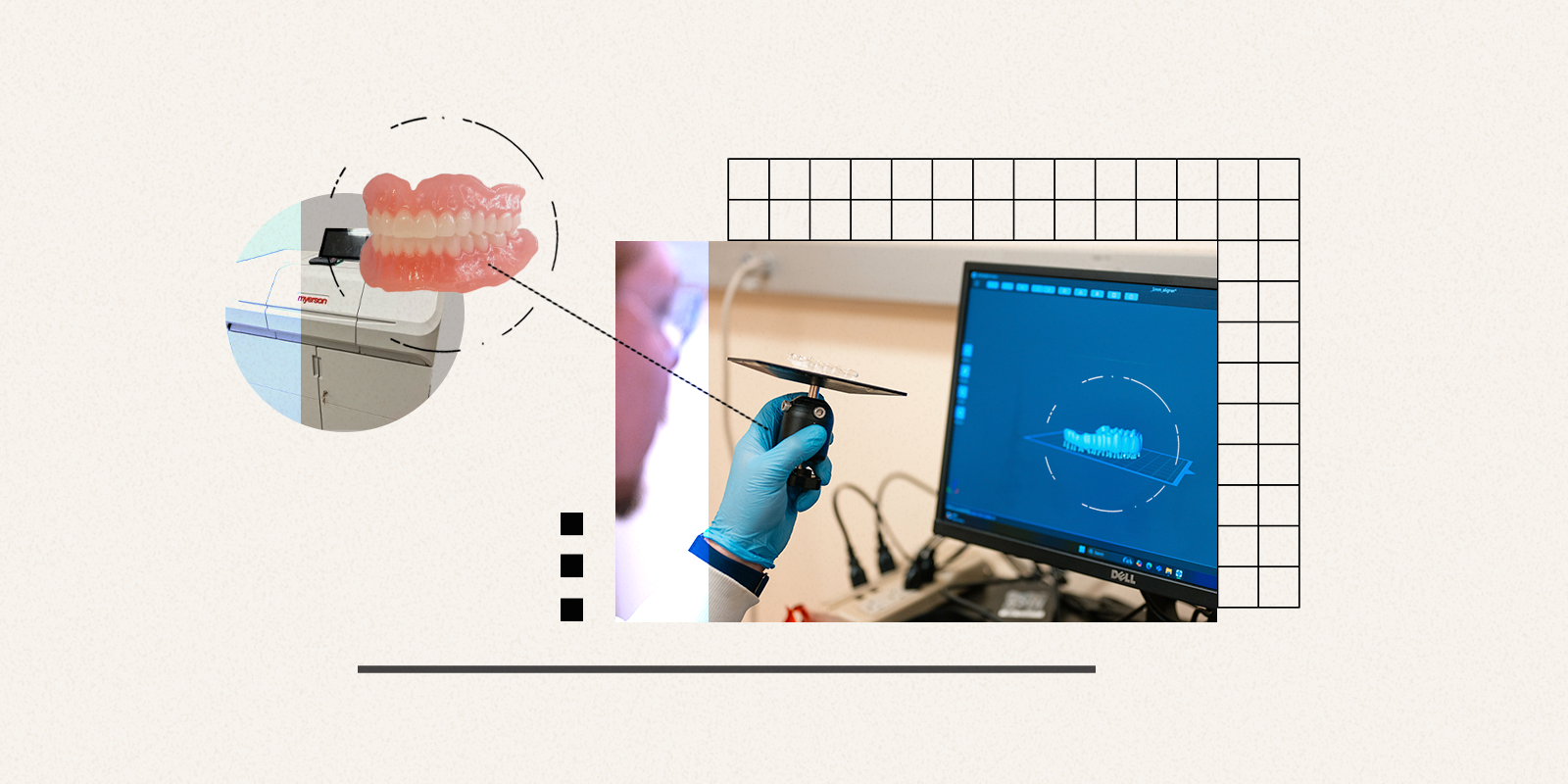
In the last ten years, we have been using a wand with a digital camera to scan the mouth, instead of taking analog impressions to create a physical mold. This helps us get the patient's tooth structure and soft tissue makeup, so we can turn that into a reverse file instantly, and then we can 3D print that model directly. And this digital image is securely added to a patient’s electronic health file, not a filing cabinet of teeth models.
That opened the door for digital dentistry on the additive manufacturing side. Rather than subtractive manufacturing via milling (a process by which material is ground away from a puck of material), now we're talking about 3D printing as additive manufacturing. This way we’re only printing the exact material needed so there's little to no waste. And now we have even more flexibility in the design aspect. Early on, models were efficiently produced but the 3D printed materials lacked the properties necessary for clinical functionality and durability in dentistry.
That's been evolving and we're now in a position where the properties of the 3D printed dentures are comparable or better than analog dentures. The milled materials have previously offered better properties but our recent work has closed that gap too.
What's being used currently to 3D print dentures is almost exclusively vat-based 3D printing with a single material. In this process, the material starts as a liquid resin contained in a vat. A patterned light is projected onto the resin—either from above or below—to cure a very thin layer of material, typically between 20 and 100 microns thick. The object is built one layer at a time. After each layer is cured, the build plate moves incrementally up or down, allowing the next layer to form. Each layer can have a unique pattern, and together these layers create the final three‑dimensional object. Using this method, it’s possible to 3D print a denture base and teeth separately. However, they still need to be bonded together.
But it is a big jump from dental models to clinically functional dentures – we needed better materials.
What’s next after vat-based 3D printing in dentistry?
We're focusing on multimaterial inkjet printing.
Rather than using single materials in the vat-based printing format to separately build the teeth and base forms, we use the inkjet process to simultaneously deliver micro droplets of either the tooth, base or support material that are jetted to just the right location for that layer. The cycles continue with putting down the materials within each layer that are immediately pinned in place under a curing light. We’re building the entire denture as one unified piece, called monolithic, rather than having to integrate separately printed or otherwise manufactured teeth with a base.
That's the distinction. It's much faster, and much stronger. We're eliminating those labor-intensive steps that still might not get the best fit for a patient. Now it’s one part, locked together at the molecular level and accurate to the patient’s mouth.
Does 3D inkjet printing allow for different materials?
Yes and we can also – for the first time – provide excellent properties from jetted inks that can be locally modified.
As a simple example: teeth have different colors, they’re not monochromatic. Now with 3D inkjet printing, we can subtly vary colors or have more translucency at the edge of the tooth versus more opacity in the body of the tooth – effectively mirroring what natural teeth look like.
This gives us the ability now to play with the digital design for both the denture base and teeth in terms of the aesthetics and the optimization of the material properties locally throughout the device. As another example, we can incorporate very stiff but high toughness materials to design thinner dentures that provide enhanced tooth support but also a more natural thermal transfer from food or drink.
Nobody has really explored these design and performance possibilities yet. Here at the CU Anschutz School of Dental Medicine, we are on the front line of this.
Where are we in the timeline of this in terms of patient adoption?
So far, our early materials have been picked up in some of the labs that do the work for dentists. A practitioner sends in a file to the lab, the lab prints the denture, and mails it out to them. That takes about a week. Some of the dental practices are considering having a printer right there in their office. It's not a cheap printer, but it allows potentially even a same-day or next-day turnaround.
This is about the lowest cost denture that you're going to see in terms of the materials and processing involved. We still rely on dentists to initiate and complete the cases. This approach to patient-specific digital denture production is extremely efficient. But what we're really after is the highest clinical performance along with that. And if we are successful, we could provide dentures to patients in communities across the state. The Advanced Clinical Training and Service (ACTS) Program at our school allows students to practice in rural and remote locations in Colorado, and this can go hand-in-hand with that program.
Are there challenges with wider adoption of 3D printed materials?
We have even better materials that we've developed and patented and are just waiting to push those forward. However, FDA clearance has to be achieved every time we change the formulation. We're confident that we'll be able to move this along to ultimately help more patients.
What are some of the things that you're trying to iterate on and are excited about?
One of the big problems with dentures is that they provide a welcoming surface for harmful bacteria and fungi to grow, often causing unpleasant odor and taste. If dentures are not thoroughly cleaned, these microbes can spread to the mouth’s soft tissues, leading to sores, inflammation and infections — and in some cases, may even be inhaled, raising health concerns beyond the mouth.
In a critical collaboration with the laboratories of Devatha Nair, PhD and Michael Schurr, PhD, the team developed a novel additive that can be incorporated into denture materials in very small proportions. Once photo-cured during 3D printing, the additive becomes an integral part of the denture that helps inhibit microbial and fungal growth.
This new approach has the potential to dramatically improve oral health for people who wear dentures. Studies done in both the laboratory and living systems have shown major reductions in harmful bacteria and fungi. While the results are very encouraging, the material will still need additional FDA approval because it actively works to protect health, rather than functioning as a standard denture material.
As the technology moves through the regulatory review process, it marks an important step forward in the development of next-generation dental materials. We’re looking at a future where when patients lose some or even all their teeth, they’ll have faster, affordable access to high-performance dentures that are more comfortable to wear and good for their oral health.
Need dentures? Read more about what it is like to get dentures at the CU Anschutz School of Dental Medicine.

.png)
.jpg)
.png)
.png)